
Pancreatic Neuroendocrine Tumor
Although this type of cancer is rare, it is essential to understand the causes and treatment options for nonfunctional pancreatic. This article will focus on the grounds of this type of tumor, the genetic studies that have been conducted, and the challenges that healthcare providers face when diagnosing and treating this type of cancer. Ultimately, this information will help you better understand the condition and find the best treatment for you.
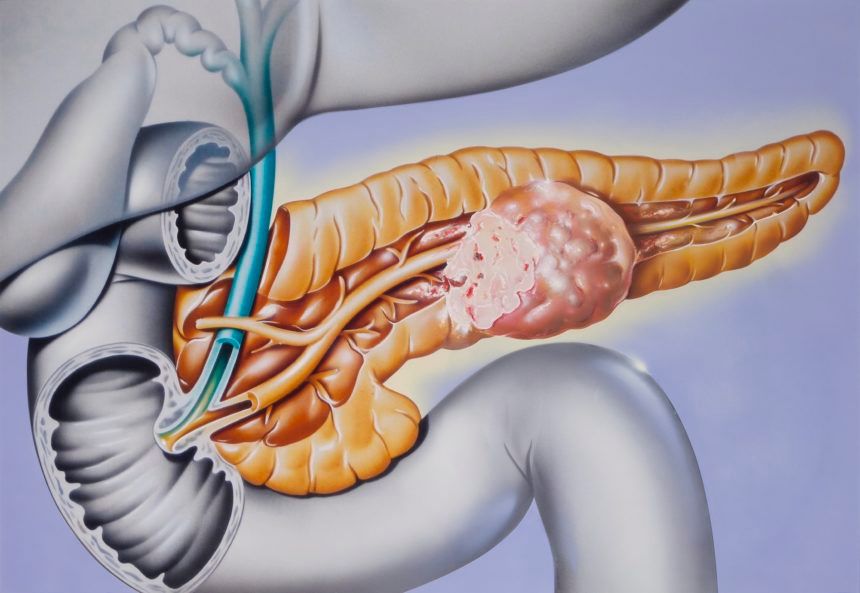
Nonfunctional pancreatic neuroendocrine tumor
A 38-year-old female presented with a nonfunctional pancreatic neuroendocrine tumor. The patient's symptoms were not exacerbated by chemotherapy and are currently under clinical follow-up.
While pancreatic neuroendocrine tumors are rare, they account for about one in every 100,000 people. They represent one to two percent of all pancreatic tumors and are considered a relatively heterogeneous group of tumors. In addition to presenting with various symptoms, they have many lineages and clinical characteristics. As a result, tumors are often misdiagnosed as other pathologies, and surgical management of these cancers should be customized to the patient's unique situation.
Genetic studies
Inherited pancreatic cancer syndromes may affect treatment decisions and the timing of subsequent manifestations. Approximately 10% of all pancreatic tumors are inherited and can include multiple endocrine neoplasia types 1 and 4, neurofibromatosis type 1, and tuberous sclerosis complex. Therefore, genetic counseling is crucial for treating pancreatic cancer, and the results of genetic tests can help in early diagnosis.
Among the new genes identified, five DEGs are highly expressed in PanNETs. The mutation frequency of these genes increased with tumor grade. Furthermore, patients with PanNETs often exhibit vascular invasion. The expression patterns of DEGs were also distinct from pancreatic ductal adenocarcinoma and were related to the vascular invasion. In addition, ABCC8 and KLKB1 co-occur on the A-D-M axis; patients with mutations in any of these genes are more likely to die from pancreatic cancer.
Treatment options
Pancreatic neuroendocrine tumors (PanNETs) arise in the neuroendocrine cells of the pancreas. Although the disease is rare, its increasing incidence is attributed to newer diagnostic and treatment modalities. While surgery remains the mainstay of treatment, systemic therapies, including chemotherapy, are also available. In addition, liver-directed therapies are also available for patients with pancreatic NETs.
Diagnosis and treatment options for pancreatic neuroendocrine neoplasms differ by type of pancreas. In the early stages, patients may have no symptoms. However, specific medical interventions may be required in cases with hormone secretion symptoms. Patients with advanced-stage PanNETs may present with tumor bulk or occult disease and require surgical resection. Alternatively, hepatic-directed therapies, such as partial hepatectomy or hepatic artery embolization, are used. In addition, chemotherapy regimens are active against pancreatic NETs.
Challenges of diagnosis
Pancreatic neuroendocrine tumors (PNETs) represent a unique neoplasm with a broad spectrum of clinical manifestations. In contrast to the more common pancreatic adenocarcinomas, pNETs typically display symptoms related to the endocrine function or mass effect. This type of tumor is difficult to diagnose, complicating early detection and treatment options. This case study describes a patient with a misdiagnosed PanNET. He presented with fever, weakness, hypercalcemia, and a pancreatic tail invasion into the spleen and gastric fundus. On further examination, the liver showed multiple enhancing lesions.
A patient's inherited genetic condition may complicate the diagnosis and management of a pancreatic neuroendocrine tumor. In addition, inherited syndromes may affect the treatment options and early detection of subsequent manifestations. For example, some people with pancreatic neuroendocrine tumors have inherited multiple endocrine neoplasia types I and IV, von Hippel-Lindau disease, tuberous sclerosis complex, or another genetic condition that causes specific cancer.



